The AARC presents a new series of lectures commemorating and honoring the legacy of President Kennedy, the inspirational meaning of his term of office, and the consequences of his assassination sixty-one years ago.
In the words of the distinguished British scholar Malcolm Blunt, “Jesus Christ, what we lost when we lost that man.”

Dr. Randy Robertson
For decades a meme in the JFK assassination has been the supposed discrepancy in the rearward extent of bone loss in JFK’s head between the doctors and nurses who attended him at Parkland Hospital and the extent of the wounds documented at BNMC. The case for the larger rearward defect was based upon Parkland eyewitness descriptions, photographically depicted in Robert Groden’s book The Killing of a President and a single erroneous measurement on the autopsy descriptive sheet filled out at Bethesda.
To put this in perspective, the argument should be between the Parkland personnel versus Dealey Plaza, the Zapruder film and the autopsy photos and x-rays. This is a classic case of eyewitness error versus the photographic documentation which exists from both before and after Parkland personnel made their individual assessments. This is not to argue that there wasn’t an exit wound in the rear of the head, just simply its extent.
This over estimation in bone loss by Parkland doctors has been used to try to convince individuals that the x-rays and photos must be fake since they differ from eyewitness observations. The pictorial display in Groden’s book has a series of Parkland personnel waving their hands behind their heads in an attempt to show how far back bone loss extended. Without a mirror they had no idea where their hands were actually placed. As such there is variability in each individual assessment. Moreover, in 1988 Nova had four physicians: Dulaney, Peters, McClelland and Jennings, view the original authenticated autopsy photos and all four found no discrepancy between what they recalled at Parkland and the autopsy photos taken at Bethesda.
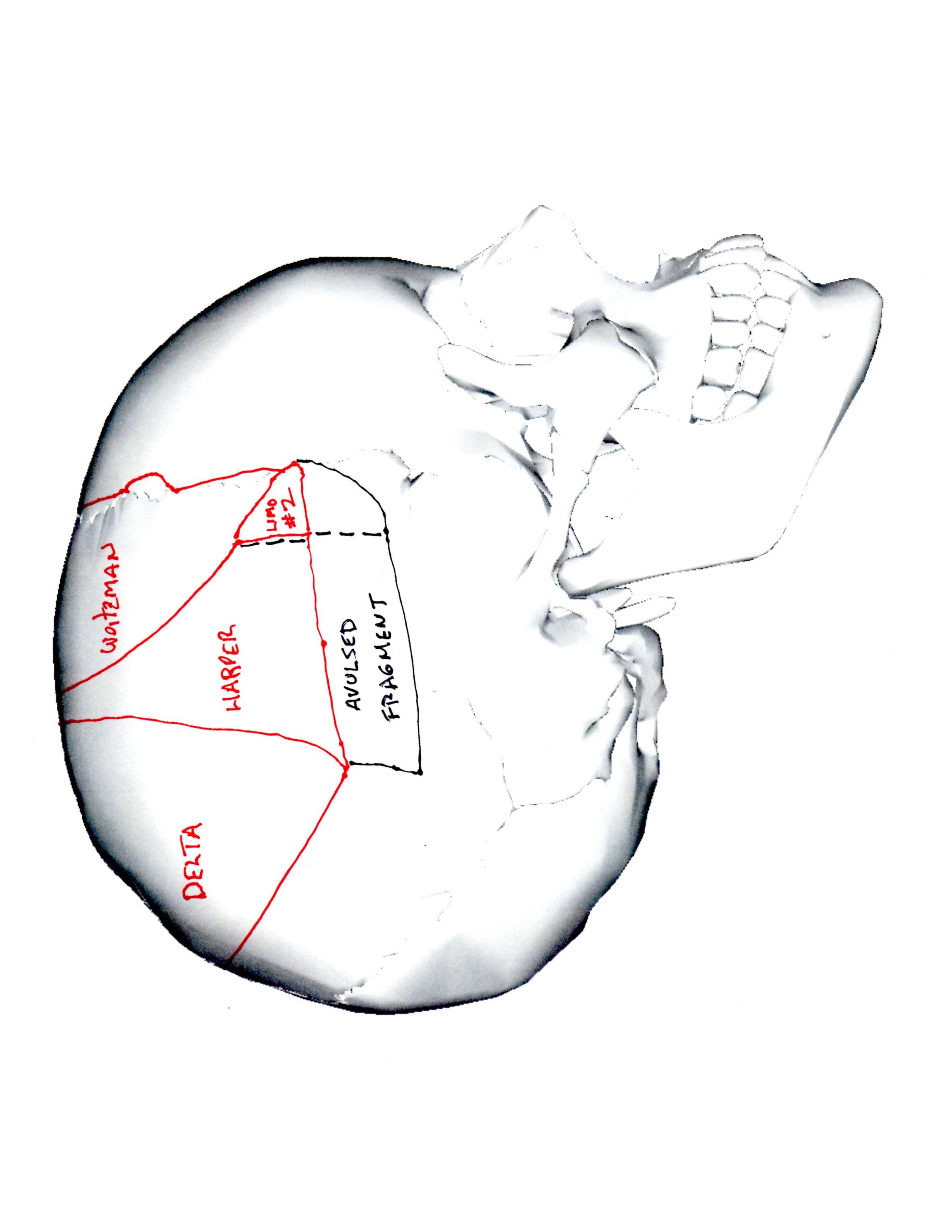
What we are assessing is bone loss and for that we can look at the Zapruder film which shows where and when skull fragments were ejected. After the first shot to the head from behind, four fragments were ejected from the mid right skull forward. The rearward extent of this initial bone loss is defined by the Harper fragment which was exploded out into Dealey Plaza, as was the more forward located Weitzman fragment. [1,2]
Harper skull fragment being ejected from JFK’s head on the Zapruder film
Weitzman skull fragment tracked after being ejected from JFK’s head out into Dealey Plaza
The Harper fragment’s origin in the right mid-parietal bone has been determined by F.B.I. photos showing characteristic arterial grooves on its inner surface which anatomically allows its placement. This is exactly where it can be seen arising on the film. This also debunks the mistaken belief that the Harper fragment is occipital bone. This assertion made by a Dallas pathologist who examined it but rendered his opinion without having seen the Zapruder film or the autopsy photos and x-rays. After this initial explosion, the rear of JFK’s head is undisturbed and no rearward expulsion of bone has occurred. [3]
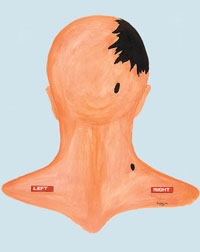
 Very shortly after another bullet struck the top rear which had been fired from the front. This is the only bullet which could have caused bone loss in the rear of the head. It is known where this bullet impacted because there is a 6.5 mm metallic particle centrally located to a series of fractures radiating outwards from this same point which is located at the top rear of the head.
Very shortly after another bullet struck the top rear which had been fired from the front. This is the only bullet which could have caused bone loss in the rear of the head. It is known where this bullet impacted because there is a 6.5 mm metallic particle centrally located to a series of fractures radiating outwards from this same point which is located at the top rear of the head.
 The impact dislodged a single large triangular skull fragment, the Delta fragment, backwards out onto the trunk of the limo.
The impact dislodged a single large triangular skull fragment, the Delta fragment, backwards out onto the trunk of the limo.


Delta skull fragment bearing an exit wound on JFK limo trunk
No other skull fragments are seen ejected from the rear. In one corner of this large fragment multiple small metallic particles were deposited from the same bullet which had left the 6.5 mm metallic particle in the top rear of the head.
In addition, there was external beveling in this same corner indicative of an exit wound. The Delta fragment determines the rearward extent of bone loss which was forward of the higher impact point. Nearly the entirety of bone loss was compromised by the total of five recovered skull fragments. [8]
 On the post-mortem skull x-rays there are no metallic particles low in the rear which could have caused lower bone loss as suggested by the Parkland eyewitnesses.
On the post-mortem skull x-rays there are no metallic particles low in the rear which could have caused lower bone loss as suggested by the Parkland eyewitnesses.
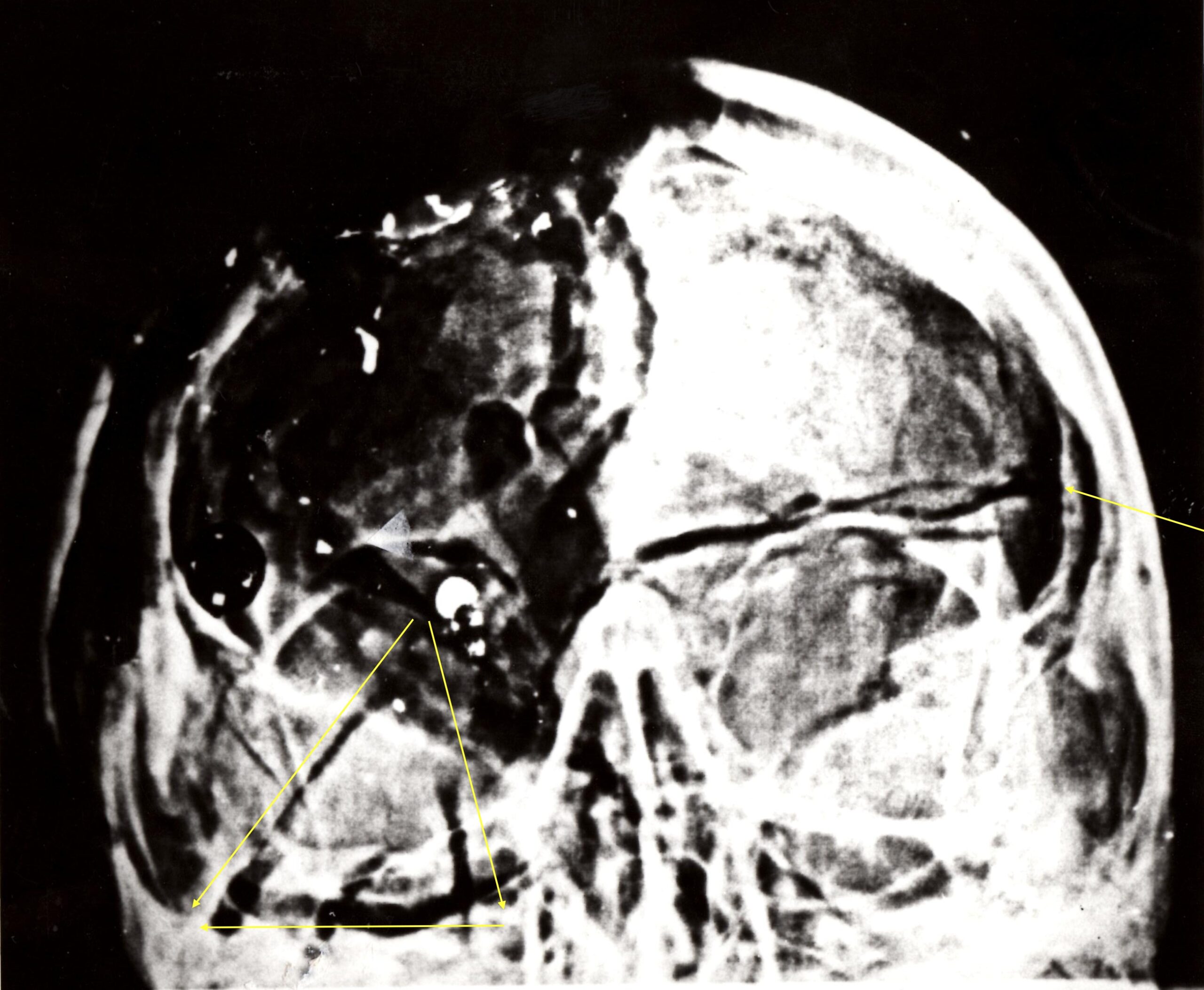
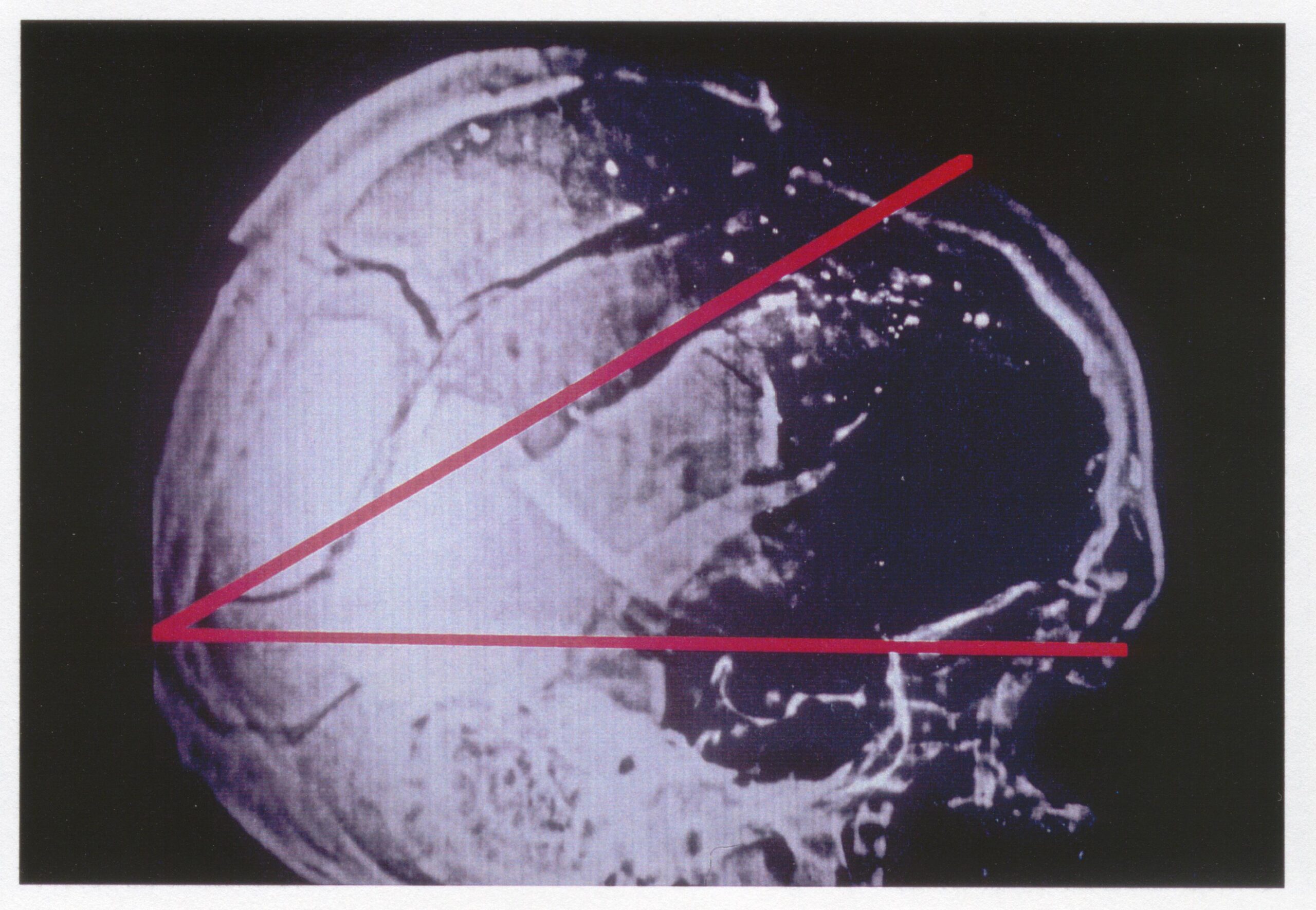
Now we can turn our attention to the findings at BNMC. The skull x-rays taken shortly after JFK’s arrival show the 6.5 mm metallic particle at the top rear with fractures radiating outward with two prominent ones, measuring 6 and 4 cm, extending downward into the still present right occipital bone. If occipital bone had been missing, you wouldn’t be able to see the fracture lines.
 The damage to the skull was diagrammed by the autopsy team and they diagrammed the 6 by 4 by 3 cm fragment of occipital bone.
The damage to the skull was diagrammed by the autopsy team and they diagrammed the 6 by 4 by 3 cm fragment of occipital bone.
 One measurement on the autopsy descriptive sheet, which has been cited as evidence for greater bone loss is a notation of “10 by 17 cm missing” with the 17 cm dimension representing the forward to rearward bone loss. If true this would indicate bone loss beneath the higher impact point. This is contradicted by the photos and x-rays showing the occipital bone to be present and by the 6 by 4 by 3 cm measurement of fractures in the right occipital bone noted on the same descriptive sheet. The apex of this triangular bone fragment can also be seen in the photos of the interior of the rear of the skull. Intact but fractured occipital bone, as seen on the x-rays, photos and the 6 by 4 by 3 cm notation is incompatible with the “10 by 17 cm missing” from front to rear. The autopsy report itself says that the greatest dimension of bone loss was 13 cm not 17 cm. 13 cm of bone loss in the anterior/posterior dimension is entirely compatible with the bone loss seen on the x-rays as well as the Zapruder film’s documentation of skull fragments lost from the wounds. The 13 cm measurement may well have been included in the notes that Humes burned. The illustrations of the damage to JFK’s head made for the Warren Commission show the occipital bone present as well.
One measurement on the autopsy descriptive sheet, which has been cited as evidence for greater bone loss is a notation of “10 by 17 cm missing” with the 17 cm dimension representing the forward to rearward bone loss. If true this would indicate bone loss beneath the higher impact point. This is contradicted by the photos and x-rays showing the occipital bone to be present and by the 6 by 4 by 3 cm measurement of fractures in the right occipital bone noted on the same descriptive sheet. The apex of this triangular bone fragment can also be seen in the photos of the interior of the rear of the skull. Intact but fractured occipital bone, as seen on the x-rays, photos and the 6 by 4 by 3 cm notation is incompatible with the “10 by 17 cm missing” from front to rear. The autopsy report itself says that the greatest dimension of bone loss was 13 cm not 17 cm. 13 cm of bone loss in the anterior/posterior dimension is entirely compatible with the bone loss seen on the x-rays as well as the Zapruder film’s documentation of skull fragments lost from the wounds. The 13 cm measurement may well have been included in the notes that Humes burned. The illustrations of the damage to JFK’s head made for the Warren Commission show the occipital bone present as well.

SS agent Roy Kellerman, from eyewitness observation at the autopsy, told the Warren Commission that there was 1 ½ to 2 inches of bone above the lower entry hole entirely consistent with the x-rays and Boswell’s 6 by 4 by 3 cm notation. The “10 by 17 cm missing” notation, contradicted by multiple other avenues of evidence, is the only item which can be cited to support bone loss low in the rear of the skull outside the varying amounts of bone loss the Parkland personnel claimed to have seen.
Given this, is there another interpretation of the “10 by 17 cm missing” notation? I believe there is. The autopsy team stated that, during their manipulation of the scalp, fragments of skull fell to the table. If the 6 by 4 by 3 cm isolated bone fragment had been one of these which fell to the table before this measurement was taken then 10 by 17 cm could have been noted as missing.
A special note should be made of a specific observation at Parkland made by the head of neurosurgery, Dr. Kemp Clark. He stated that both cerebral and cerebellar tissue was seen extruding from the head wound. The bullet fired from behind entered just above the cerebellum and while there are no metallic fragments low in the rear of the skull, as this was a jacketed bullet, the temporary pressure cavity created by this bullet’s passage could have disrupted cerebellar tissue. This has nothing to say about the absence of occipital bone as its presence is well documented on the post-mortem skull x-rays. The photographs taken of JFK’s brain show the cerebellum to be intact; however, the photos have no identification to say that this is JFK’s brain. If Dr. Clark was correct than the photos are not of JFK’s brain and if the photos are genuine then Dr. Clark was mistaken. This can never be resolved. What can be stated definitively is that the occipital bone was fractured but still present.
The meme of occipital bone loss, based solely on eyewitness observations and a single erroneous measurement on a descriptive sheet, refuted by the authenticated photos and x-rays as well as other notations on the descriptive sheet, should be relegated to the trash heap of JFK research. Just as a bullet hole in the windshield, that there was an entry wound in JFK’s throat, and that the Harper fragment being occipital bone should be as well. These mistaken claims only cause unnecessary confusion among neophytes to the JFK assassination and gullible individuals who have not looked at all the evidence in its entirety. Further, these claims promote the mistaken belief that much of the valid hard evidence has been faked. This is completely counterproductive to a full understanding of the nature of the head wounds which proves conspiracy.
Copyright © AARC. All rights reserved.
Randolph Robertson M.D.
AARC Board Member
Randolph Robertson M.D. has researched the assassination of President Kennedy for more than 25 years. He holds B.S. and M.S and M.D. degrees from the University of Illinois at Champaign-Urbana. Dr. Robertson is a Board-certified Diagnostic Radiologist and is one of very few medical professionals outside of governmental review panels to have been given permission via the Kennedy family to see and review the original autopsy materials held at the National Archives. He has testified before the House of Representatives Legislation and National Security Subcommittee on Government Operations on the Effectiveness of the President John F. Kennedy Record Collections Act of 1992 in November 1993 in Washington DC.
He presented his analysis of the post-mortem radiographs at the annual meeting of the National Association of Medical Examiners in September of 1993 in Fort Worth Texas. More recently he presented his synchronization of the Zapruder film and the Dallas Police Department DictaBelt at the LeftForum meeting in 2014 in New York City. He is currently retired from practicing in radiology.
